
Treatment Planning is NOT “One Size Fits All”
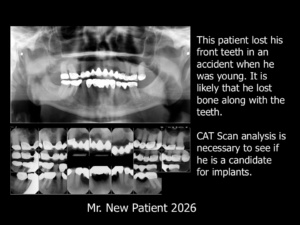 Last month Mr. “New Patient” visited me to obtain an opinion about what he should do with his mouth. Mr. New Patient is in his sixties. His existing bridgework is stable and he is comfortable. This bridgework is his second full arch upper restoration since the accident that knocked out all of his front teeth when he was a teenager. The X-Rays reveal a decayed bicuspid completely separated from his full arch upper fixed bridge. The remaining posterior teeth appear to be sound, with nice, long roots and excellent periodontal bone.
Last month Mr. “New Patient” visited me to obtain an opinion about what he should do with his mouth. Mr. New Patient is in his sixties. His existing bridgework is stable and he is comfortable. This bridgework is his second full arch upper restoration since the accident that knocked out all of his front teeth when he was a teenager. The X-Rays reveal a decayed bicuspid completely separated from his full arch upper fixed bridge. The remaining posterior teeth appear to be sound, with nice, long roots and excellent periodontal bone.
Mr. New Patient visited several dentists—all of whom recommended that he extract all of his posterior teeth and restore his upper arch with four implant fixtures and an “All-on-Four” case. An All-on-Four case consists of four implant fixtures (usually two in the front and two in the back) with a denture-like restoration screwed into them.
I suspected that Mr. New Patient may not be a good candidate for implants. It is likely that substantial anterior bone was lost in the accident along with his front teeth. It is difficult to ascertain whether Mr. New Patient is a good candidate for implants based on the full series of X-Rays and panorex pictured here. As a result, I requested that an oral surgeon conduct a CAT scan analysis and provide an assessment. If Mr. New Patient turns out not to be a good candidate for implants in the front of his mouth, it is reasonable to conclude that he would also have a poor prognosis for an All-on-Four case.
About the All-on-Four Case
A major drawback of All-on-Four cases is that implants often are not placed in the bone with enough depth to provide adequate support for the full arch restoration. All-on-Four restorations usually consists of a single, large, denture-like superstructure that not only replaces the missing teeth, but the missing gingiva and bone as well. Often the restoration is designed so that it is impossible for patients to adequately clean around the implant fixtures and under the pontic areas.
Implantology experts, such as Dr. Carl Misch, warn against overloading implant fixtures with large superstructures. After years of painstaking research, he developed a Stress Treatment Theorem, which states that “treatment related to the science of implant dentistry should be centered around the biomechanical management of stress.1”
Implants and their restorations are feats of engineering, and ALL engineering structures—whether they support bridgework across a river or bridgework in the mouth–cannot be overloaded with forces or they will fail. There are numerous examples of bridge failures in the civil engineering world that failed as a result of overloading with forces. A perfect example is the collapse of the Schoharie Bridge on the New York State Thruway in 1987.2 The support columns for this bridge were sunk into riverbed sand. Over time, the sand washed away from the support columns through a process called scour. The supports were no longer able to support the bridge span, and it collapsed, resulting in deaths.
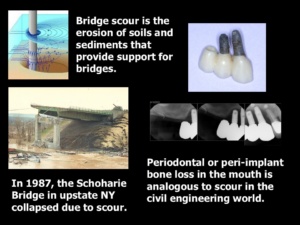 In a mouth restored with implant-supported bridgework, scour is analogous to the disappearance of the peri-implant bone. The bone around implants—just like the sand around the Schoharie Bridge supports—can disappear as a result of overloading with forces. When most of the peri-implant bone vanishes, the implants become loose and exfoliate. It is not unusual for the entire restoration to fall out with the failed implants. Dr. Misch emphasized in his years of ground-breaking research that there is a strong correlation between peri-implant bone loss and overloading implant fixtures.
In a mouth restored with implant-supported bridgework, scour is analogous to the disappearance of the peri-implant bone. The bone around implants—just like the sand around the Schoharie Bridge supports—can disappear as a result of overloading with forces. When most of the peri-implant bone vanishes, the implants become loose and exfoliate. It is not unusual for the entire restoration to fall out with the failed implants. Dr. Misch emphasized in his years of ground-breaking research that there is a strong correlation between peri-implant bone loss and overloading implant fixtures.
As far as I can determine, the All-on-Four concept has no proven track record for longevity. I have yet to see one presentation or published article that documents the longevity of these cases. Practitioners seem pre-occupied with inserting esthetic cases in as few visits as possible to maximize the monetary remuneration and minimize overhead. They seem oblivious to potential consequences that could arise as a result of overloading the implant fixtures.
The sad reality for All-on-Four cases is that if the implants fail, the patient will really suffer. Additional implant placement may not be possible or may require extensive surgical procedures and bone grafts. Worse still, the bony ridges in an All-on-Four case are flattened. Flattened ridges make it difficult or impossible to comfortably wear a denture.
Despite these drawbacks—and the fact that there are better treatment alternatives—the All-on-Four case seems to be the only choice patients are offered these days. A major reason is that this treatment option seems to be the only choice most dental practitioners can offer.
What is clear from the X-Rays and from examination is that Mr. New Patient’s posterior teeth offer a solid foundation for dentistry. Why should they be extracted? These teeth have excellent periodontal bone and long roots. They have successfully supported full arch bridgework for decades. I could easily restore all of Mr. New Patient’s posterior teeth, including the bicuspid that separated from the bridgework.
Dental Researchers Giannobile and Lang observed that “the long-term prognosis for implants has been shown to be far less promising than that for natural teeth, even when they are compromised by periodontal disease or endodontic problems…Often practitioners recommend implants even when teeth are only modestly compromised by caries, the need for endodontic therapy, or periodontal disease to provide the patient with a quick solution to the problem. Less trained individuals often recommend tooth extraction rather than retention. This condemns many teeth that could be treated and returned to good function. Even those teeth that are compromised have a much greater life span than the average implant.3”
It is important to understand that patients go to the dentist to save their teeth, not to have implants. Except in certain circumstances (such as congenitally missing lateral incisors), implants should be a last resort, rather than a first resort.
So, what else can be done for Mr. New Patient aside from “All-on-Four”?
Alternative Treatment Options
It would never occur to most dental practitioners that Mr. New Patient has at least three other restorative choices aside from All-on-Four. These choices are far less invasive and offer a far better prognosis for success. Here are the choices:

- Anterior Implant Bridgework with Posterior Bridgework on Natural Teeth: If Mr. New Patient is a good candidate for implants, three implants can be placed in the anterior region—ideally two in the canine positions and one in a central incisor position to make a fixed anterior bridge. The posterior teeth can be restored with conventional bridgework. The implants should be placed in the proper position with ideal emergence profile so that the patient can maintain the bridgework. The bridgework should be made sleek (like the adjacent example). It is good practice to make metal lingual surfaces so that the bridgework can be as sleek as possible to minimize the load on the implant fixtures.
Dental practitioners must accept that implant-supported fixed bridgework is more about function than about esthetics. If too much gingiva and bone must be added to adequately support the lip, the implant fixtures are likely to be overloaded with forces and difficult to maintain hygienically. In this scenario, removable bridgework of some kind is a better treatment option than implant-supported fixed bridgework. If implants of adequate depth cannot be placed in the upper anterior region of the mouth to support a fixed restoration, then this treatment option cannot be recommended.
It is worth noting that Mr. New Patient has the choice to do nothing—to wait until his upper arch restoration completely fails and then opt for extracting the remaining teeth and placing a denture. This option is not recommended because Mr. New Patient has the opportunity to save his posterior teeth with two treatment options that would provide far more comfort than a denture:

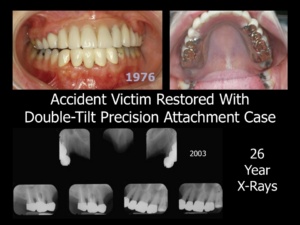
- Double-Tilt Anterior Precision Attachment Case4: The Double-Tilt Precision Attachment Partial Denture case has one of the best track records in Dentistry. These cases last longer than the fixed bridgework cases. Unfortunately, the “powers that be” seem to have successfully blotted this treatment option from collective memory. The Double-Tilt concept was invented in 1906 and can be employed with both natural tooth and/or implant abutments. Double-Tilt Precision Attachment cases last far longer in health than any other type of full arch restoration. They are documented to last for decades on the worst teeth imaginable.
The reason why the Double-Tilt Precision Attachment case is so successful is that the Double-Tilt Precision Attachment case functions vertically and does not inflict destructive lateral forces on the abutments. The attachment consists of a simple male-female with no locking or gripping mechanism. Retention is created by the path of insertion, which is tilted in two directions: an antero-posterior tilt and a mesio-distal tilt. This path is different from the pull of the muscles and gravity. If a stress is applied to the removable prosthesis, it can move slightly to relieve the stress, but it cannot dislodge. The Double-tilt precision attachment removable is worn 24 hours a day and does not require powder or paste. The only maintenance required (aside from hygiene) is an occasional reline or replacement of acrylic teeth/occlusion. Unlike attachments that grip or lock the removable in place, male/female attachments employed in this manner rarely require replacement, even after decades of continuous wear!
Mr. New Patient is an excellent candidate for a Double-Tilt Precision Attachment case—no implants required! As the illustrations demonstrate, the double-tilt precision attachment case has proven to be successful for cleft palate patients and accident victims who are not candidates for implant therapy. Most professionals have a built-in bias against removable restorations because they have experienced difficulties with removable restorations. Unfortunately, they are not familiar with the Double-Tilt Precision Attachment Partial Denture, which is completely unlike any other type of removable partial denture. Practitioners should understand that fixed bridgework is not always superior to removable bridgework.

- Full Arch Fixed Bridgework with Overlay Connection of Right and Left segments: One fact is clear: the patient has already worn fixed bridgework successfully on these abutment teeth for decades. There is a very good possibility that fixed bridgework could succeed on these teeth for many more years—especially if the decayed bicuspid can be salvaged (which I believe it can be). Because of the large span, the patient must be willing to accept responsibility for transitioning to a different kind of case should that become necessary.
However, the type of roundhouse bridgework that was made in the past should NOT be fabricated in the same way for several reasons:
1. Parallelism: Restorative dentistry must be made with precision in order to have the most successful outcome. It is impossible to prepare teeth on opposite sides of an arch so that all the teeth are parallel for the precise fit of a one-piece full-arch restoration. There is a big difference between a restoration that fits with precision and a restoration that “goes on.”
2. Manufacturer’s Directions. Manufacturers explicitly warn that Porcelain-to-Metal Bridgework should not be designed as one-piece roundhouses because dimensional changes are inevitable with repeated heating close to the melting point. When fabricating full arch dentistry, these changes are significant and can affect the fit and overall case outcome.
3. Contingency Plan. The use of an overlay (telescoping) to connect right and left segments circumvents the problem of dimensional changes in roundhouse restorations. An overlay design offers a contingency plan in the event that something goes wrong. The overlay can be removed to address problems or transition to a different type of case without remaking any of the underlying posterior restorations. With the overlay approach, recurrent decay is not a concern because the abutments are protected with an underlying layer of metal. The illustrated case demonstrates that long-span bridgework can be successful when there is a strong foundation, excellent periodontal bone and long roots.
Choosing the Right Treatment Option
Mr. New Patient’s case illustrates beautifully that determining the right treatment option for a complex case is not a simple task. Patients are individuals, with unique needs, medical histories and desires. “Just making the right treatment choice among the many options can be difficult—even for expert clinicians,” explains Dr. Atul Gawande in his book The Checklist Manifesto.5”
As noted, dental practitioners today do not have enough treatment options in their treatment armamentaria to consider. In addition, clinicians rarely spend enough time analyzing complex cases. As a result, most practitioners unknowingly set themselves up for less-than-ideal outcomes or outright failures.
Lisa Sanders, in her book Every Patient Tells a Story,6 points out three causes of errors that doctors make unwittingly:
*Faulty synthesis: difficulty analyzing and interpreting the collected data and knowledge to come up with the best treatment option.
*Premature Closure: latching on to particular treatment option and closing off the consideration of alternatives.
*Diagnostic Momentum: labelling patients with a definite diagnoses and treatment options as a result of biases, distorted thinking and blind spots.
When snap decisions are made, critical thinking goes out the window and mistakes happen. Doctors must avoid yielding to “groupthink” biases and prejudices. They must also guard against succumbing to patient demands to come up with an instant plan and price. Patients often do not understand that the doctor is acting in their best interest by taking time to thoroughly analyze their cases and by consulting with specialists for additional information. As the great poet Alexander Pope (1688-1744) once said, “fools rush in where angels fear to tread.7”
Critical Thinking
 The famous physicist Richard Feynman remarked in an interview8 that “most people don’t actually think, they accept.” Dr. Feynman is famous for his out-of-the-box thinking to solve problems that his colleagues with far higher IQs could not solve. His ingenious approach to solving problems won him the Nobel Prize for quantum physics. Dr. Feynman emphasizes that “thinking isn’t a talent you are born with; it is a habit you build.”
The famous physicist Richard Feynman remarked in an interview8 that “most people don’t actually think, they accept.” Dr. Feynman is famous for his out-of-the-box thinking to solve problems that his colleagues with far higher IQs could not solve. His ingenious approach to solving problems won him the Nobel Prize for quantum physics. Dr. Feynman emphasizes that “thinking isn’t a talent you are born with; it is a habit you build.”
So how do you train your brain to think instead of accept? Dr. Feynman trained his brain to think by always translating whatever he learned into “something [he] could see or touch or imagine.”
Dental Practitioners should do the same. They should diligently learn what treatment options are available for a particular dental condition, as well as the pros and cons of each option. They should have a team of top-notch specialists they can consult to gather appropriate information and to discover what specialists can do for their patients. An Oral Surgeon who is placing implants routinely can best determine whether or not a patient is a good candidate for implants.
In other cases, orthodontics might be necessary to achieve an ideal result. Consulting with an orthodontist could identify the best possible treatment option. I have always met in person with orthodontists on behalf of my patients. I did so when I practiced dentistry in NY and I continue to do so now that I am in practice in Arizona. I bring models, pictures, and X-Rays to our meeting, and often we meet over lunch. I pass the information to my patient when I present the treatment options. Patients are impressed that I took time out of my busy schedule to meet in person with a specialist on their behalf. They look at me as being completely different from other dentists. The orthodontic specialists also look at me differently. Very few of their referring doctors ever take the time to meet with them in person to inquire about a patient.
“Critical thinking is rebellion in a world that fears individuality,” says writer and “thinker” Roneil Cole says in his article The Death of Critical Thinking And Why We Must Revive It Now9. “It’s the ability to dissect information, weigh evidence, recognize bias, and challenge your own assumptions.”
“Reviving critical thinking doesn’t require a PhD,” he concludes. “It requires the courage to slow down, to listen, and to question.”
Thinking critically means asking questions such as these:
- Are there anatomical limitations that will result in poor outcomes for certain treatment options (such as implants)?
- What options offer the least invasiveness and the best prognoses?
- If I (or my family member) had the patient’s problem, what treatment would I want for myself?
- What treatment option would be the best recommendation for a patient considering the patient’s needs, desires and medical history?
- Is there a built-in contingency plan in the event of a complication (such as the loss of a weak abutment) so that the entire case is not jeopardized?
 Critical thinking means not yielding to “groupthink” or personal biases to quickly formulate a complex treatment plan. It means listening to the patient and having a frank discussion about the pros and cons of each treatment option. It is not the doctor’s job to tell patients what to do. “Doctor” means teacher, and it is the doctor’s job to educate patients and help them make the treatment choice that is right for them.
Critical thinking means not yielding to “groupthink” or personal biases to quickly formulate a complex treatment plan. It means listening to the patient and having a frank discussion about the pros and cons of each treatment option. It is not the doctor’s job to tell patients what to do. “Doctor” means teacher, and it is the doctor’s job to educate patients and help them make the treatment choice that is right for them.
“All of this takes time,” says Dr. Jerome Groopman, author of How Doctors Think.10 “Those who see medicine [dentistry] as a business rather than a calling push for care to be apportioned in fixed units and tout efficiency. A doctor’s office is not an assembly line. Turning it into one is a sure way to blunt communication, foster mistakes, and rupture the partnership between patient and physician [dentist]. A doctor can’t think with one eye on the clock and another on the computer screen…Complicated problems cannot be solved in a rush. The inescapable truth is that good thinking takes time. Working in haste and cutting corners are the quickest routes to cognitive errors.”
To Summarize:
When analyzing a complex case:
- Conduct the appropriate diagnostic tests and make sure that these tests were done properly.
- Create a thorough diagnosis: write down every abnormality, including the patient’s medical and dental history.
- Listen carefully to the patient’s story as well as perceived needs and desires.
- Make a list of possible treatment options and think about the pros and cons of each one.
- Consult specialists to find out what they could do for the patient. Their reports will help identify the best treatment option.
- Take time to determine which treatment option you would personally recommend for that patient.
- Present the possible treatment options to the patient and thoroughly discuss the pros and cons of each option, as well as the treatment option you recommend.
- Show the patient similar cases and how they lasted in health.
- Guard against snap judgments, clinical biases and yielding to time pressure. Don’t be afraid to bring the patient back for additional consultation visits if appointment time runs out. There should be no rush to come up with an ultimate answer in a complex case. Time spent talking to patients at the outset will go a long way toward preventing problems later on. As Benjamin Franklin famously observed, “An ounce of prevention is worth a pound of cure.11”
1Carl E. Misch, BS, DDS, MDS, PhD (hc); “The Key to Implant Treatment Plans: Stress Treatment Theorem for Implant Dentistry;” Implant Prosthodontics Monographs; Vol. 1, No. 2; June 2017.
2https://en.wikipedia.org/wiki/Schoharie_Creek_Bridge_collapse
3Dental Abstracts Vol 61, Issue 4; 2016; p.173; Keep the Ones Youve Got; Giannobile, WV, Lang NP: Are dental implants a panacea or should we better strive to save teeth? J Dent Res 95:5-6, 2016. 2Per-Ingvar Brånemark, The Osseointegration Book: From Calvarium to Calcaneus; Editorial Board
4Feinberg, Edward; The Double-Tilt Precision Attachment Case for Natural Teeth and Implants; 2015; available on Amazon.com: https://tinyurl.com/3bezvm9m
5Gawande, Atul; The Checklist Manifesto: How to Get Things Right, Metropolitan Books, Henry Holt and Co.; New York; 2009; p. 10.
6Lisa Sanders, MD Every Patient Tells a Story: Medical Mysteries and the Art of Diagnosis; Broadway Books, a division of Random House, New York 2009, p. 198-213.
7Pope, Alexander; “An Essay on Criticism,” 1711.
8Interview with Dr. Richard Feyman: https://www.facebook.com/watch/?mibextid=wwXIfr&v=885089097458062&rdid=jyfYSXtGxBecRYPq
9Cole, Roneil; “The Death of Critical Thinking And Why We Must Revive It Now;” Oct 19, 2025; https://roneilcole.substack.com/p/the-death-of-critical-thinking-and
10Groopman, Dr. Jerome; How Doctors Think; Mariner Books (Houghton Mifflin Company); New York, 2007; p. 268.
11Letter to the Pennsylvania Gazette about fire prevention, 1735.

You may also like
