Chase Excellence with Sound Principles of Engineering
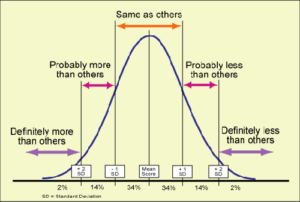 “Doctors like to think they’re doing their job as well as it can be done.,” says Atul Gawande, a noted author of medical best-sellers [“The Bell Curve,” New Yorker Magazine, November 28, 2004]. Everyone believes they are at the top of the bell curve. “But when you measure their results, the spread is wide.”
“Doctors like to think they’re doing their job as well as it can be done.,” says Atul Gawande, a noted author of medical best-sellers [“The Bell Curve,” New Yorker Magazine, November 28, 2004]. Everyone believes they are at the top of the bell curve. “But when you measure their results, the spread is wide.”
From what I can see, most dentists do not have a clue as to where they actually stand on the Bell Curve. Very few understand where full coverage restorative dentistry came from; the incredible feats that have been achieved in the past; and the “magic” that is actually possible. This knowledge is conspicuously absent from dental school curricula and postgraduate seminars.
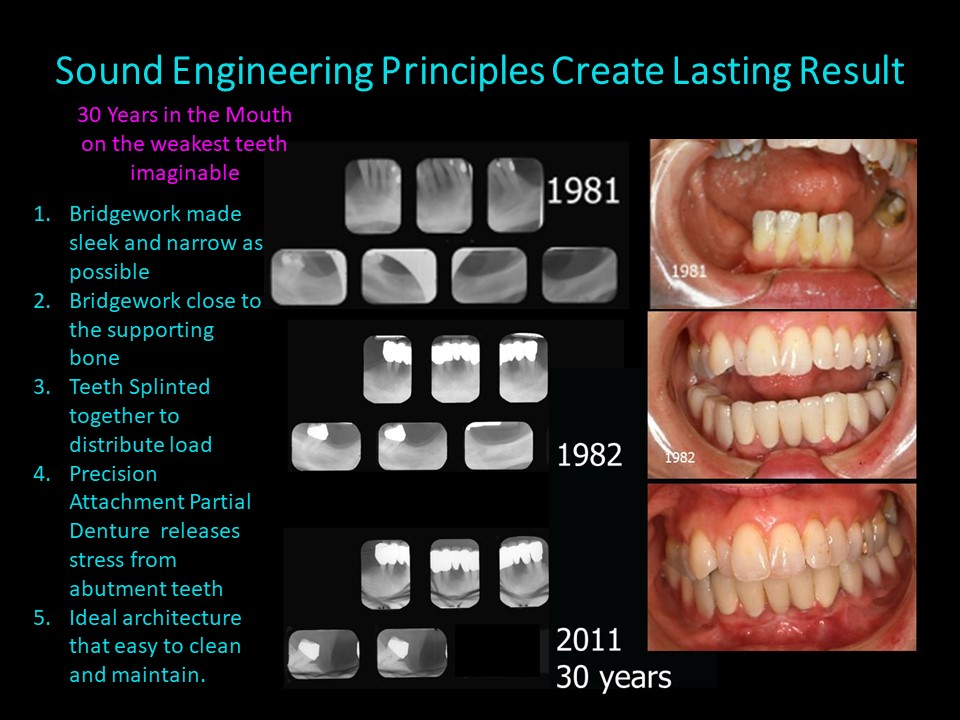
Sadly, most seminars appear to be centered around techniques with short cuts, methods of minimizing expenses and showcasing beautiful cosmetic results on the day of insertion. The patients all seem to be young with healthy gingiva. Rarely do attendees get to see whether those cases were actually successful. Did they actually last? Would those techniques work on patients with heart disease, cancer or diabetes? Would they work on a weak mouth like the case shown above? Almost never do attendees see finished X-Rays and rarer still are follow-up X-Rays 5, 10, 15, 20, 30 or 40 years later. Without longevity should those restorative techniques even be advocated? I think not.
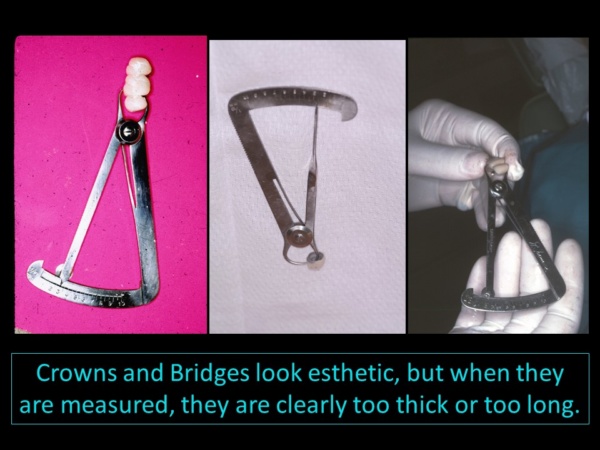 I often watch dental audiences at seminars and it is clear that very few dentists are really evaluating what they are seeing. There is no doubt that the cosmetic improvements are impressive. But very few attendees notice that finished cases—almost without exception—wind up with teeth that are larger than the original.
I often watch dental audiences at seminars and it is clear that very few dentists are really evaluating what they are seeing. There is no doubt that the cosmetic improvements are impressive. But very few attendees notice that finished cases—almost without exception—wind up with teeth that are larger than the original.
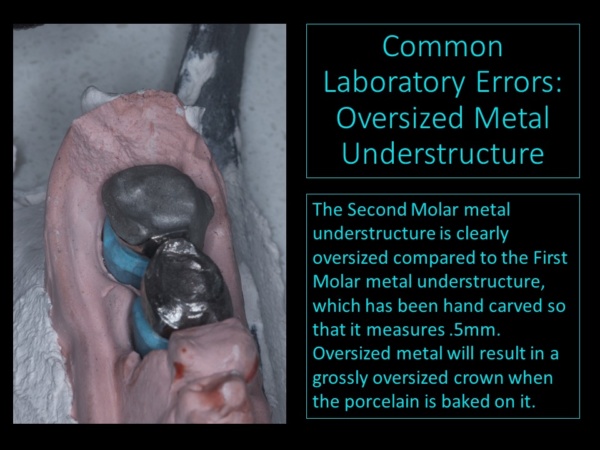
It might shock you to know that a visit to most dental laboratories with an Iwansen gauge (calipers) would reveal that the majority of the restorations on the workbenches are either too thick or too long. Common sense dictates that if only 1.0 to 1.5mm of tooth structure can be removed from a vital tooth during the preparation stage, the finished restorations should not be larger. It is not prudent to overload the foundation—roots and supporting bone–with oversized restorations.
Oversized restorations can interfere with normal function and introduce destructive habits and pain syndromes. Patients who are susceptible to periodontal bone loss are also likely to experience continued periodontal problems with oversized restorations. Since there are many other factors that can initiate periodontal problems (i.e. heart disease, cancer and diabetes), no one can be sure if a normal patient will someday become susceptible to periodontal bone loss. Oversized restorations in patients who are medically compromised can quickly turn into a nightmare.
 It is important to understand that full coverage restorations in the mouth are engineered structures. All engineered structures must effectively withstand and dissipate forces in order to last in health. The engineering world is replete with spectacular failures of bridges and buildings that did not properly take into account the forces that would be applied to those structures.
It is important to understand that full coverage restorations in the mouth are engineered structures. All engineered structures must effectively withstand and dissipate forces in order to last in health. The engineering world is replete with spectacular failures of bridges and buildings that did not properly take into account the forces that would be applied to those structures.
Abutments supporting bridgework restorations are essentially no different from the abutments supporting that bridge across the river. Both are subject to the same basic principles of engineering. Engineering failures on highway and railway bridges are quite common. Equally common are engineering failures on dental bridgework that is supported by both natural tooth and implant abutments. “Weak abutments are the most common cause of arch bridge failures,” says Mario Salvadori in his book Why Buildings Fall Down.
Sound engineering dictates that dental practitioners strive to fabricate restorations that are smaller than the original dentition—i.e. narrower bucco-lingually and perhaps shorter incisally. Sound engineering also dictates that dental practitioners strive to bring the forces as close to the supporting structures (roots and bone) as possible. The goal is to compensate for existing bone loss in order to prevent further bone loss.
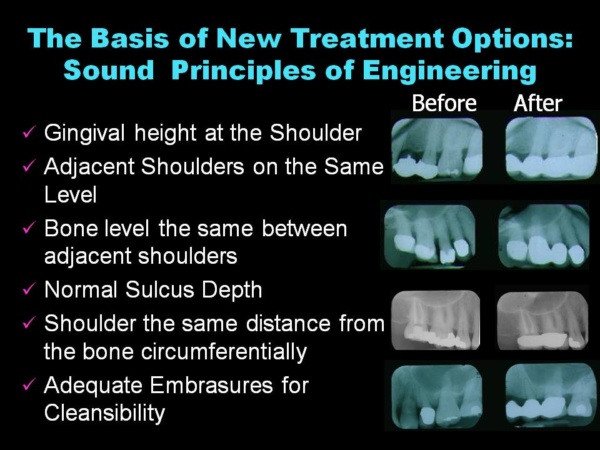
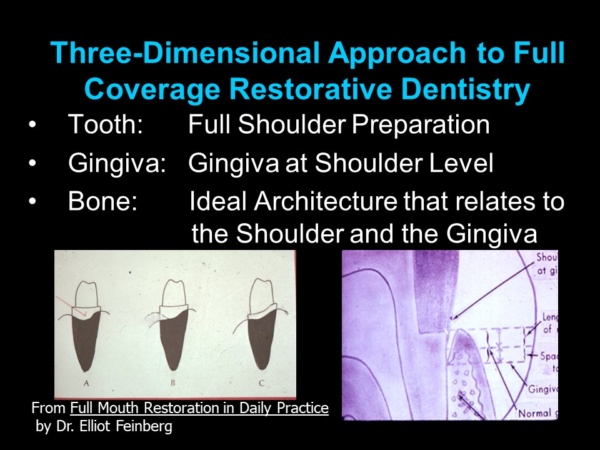 How can this be accomplished? First, teeth must be prepared three-dimensionally so that the tooth preparations relate to the gingiva (gum) and the underlying bone with ideal architecture. This approach is not taught in any dental school. All deformities must be eliminated–any edematous inflammatory tissue, and pockets must be removed and any abnormal bony defects corrected. The teeth are prepared with a flat circumferential shoulder (ledge) perpendicular to and equidistant from the underlying bone. The shoulder brings forces closer to the bone instead of all the forces being concentrated on the occlusal (top) surface. This practice actually stabilizes weak teeth in their sockets and helps loose teeth tighten up. If the foundation is weak with short, conical roots (like the case on the cover of this blog), connecting or splinting them together distributes the forces among them, so individual teeth do not have to absorb forces independently. Splinting teeth prevents individual teeth from moving out of alignment and creating food impaction areas, a known cause of periodontal breakdown.
How can this be accomplished? First, teeth must be prepared three-dimensionally so that the tooth preparations relate to the gingiva (gum) and the underlying bone with ideal architecture. This approach is not taught in any dental school. All deformities must be eliminated–any edematous inflammatory tissue, and pockets must be removed and any abnormal bony defects corrected. The teeth are prepared with a flat circumferential shoulder (ledge) perpendicular to and equidistant from the underlying bone. The shoulder brings forces closer to the bone instead of all the forces being concentrated on the occlusal (top) surface. This practice actually stabilizes weak teeth in their sockets and helps loose teeth tighten up. If the foundation is weak with short, conical roots (like the case on the cover of this blog), connecting or splinting them together distributes the forces among them, so individual teeth do not have to absorb forces independently. Splinting teeth prevents individual teeth from moving out of alignment and creating food impaction areas, a known cause of periodontal breakdown.
Structures in the engineering world are of similarly constructed. “Most of the bridges in the world,” explains Mario Salvadori, “are structured by 3 dimensional frames consisting of floor slabs supported by beams, beams supported by columns, columns supported by foundations…”
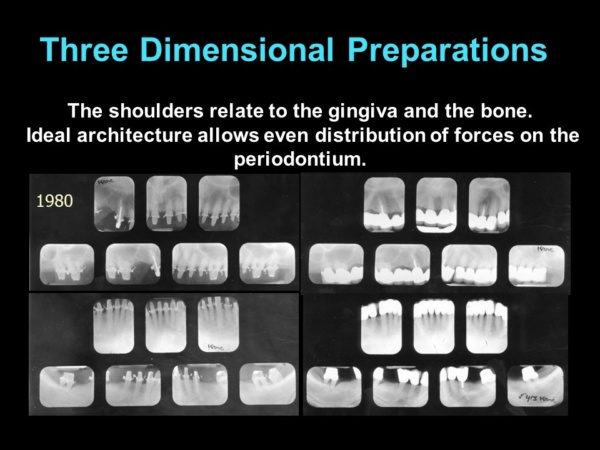 The engineered approach for full coverage restorations adopted by the ONWARD program has a 70-year track record of success and a high percentage of longevity—even after decades of continuous use, wear and tear. The X-Rays show definitively that the forces are brought as close to the bone as possible because the restorations in finished X-Rays look as if they are actually sitting on the bone. (No, they do not violate biologic width, and the reasons why are thoroughly covered in the ONWARD courses). This is not the case with the X-Rays of more than 90% of practicing dentists. Most restorations are not corrective; they are tooth “coverings” that are often far away from the bone and even supra-gingival.
The engineered approach for full coverage restorations adopted by the ONWARD program has a 70-year track record of success and a high percentage of longevity—even after decades of continuous use, wear and tear. The X-Rays show definitively that the forces are brought as close to the bone as possible because the restorations in finished X-Rays look as if they are actually sitting on the bone. (No, they do not violate biologic width, and the reasons why are thoroughly covered in the ONWARD courses). This is not the case with the X-Rays of more than 90% of practicing dentists. Most restorations are not corrective; they are tooth “coverings” that are often far away from the bone and even supra-gingival.
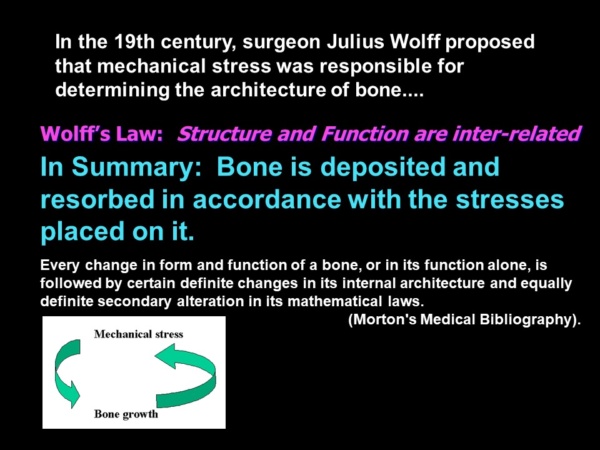 The application of scientific engineering principles to crown and bridgework is called corrective dentistry because the dental restorations are designed to minimize or eliminate the progression of periodontal bone loss. The reason corrective dentistry works is attributable to Wolff’s Law, which states that bone is deposited and resorbed in accordance with the stresses placed upon it.
The application of scientific engineering principles to crown and bridgework is called corrective dentistry because the dental restorations are designed to minimize or eliminate the progression of periodontal bone loss. The reason corrective dentistry works is attributable to Wolff’s Law, which states that bone is deposited and resorbed in accordance with the stresses placed upon it.
It is a myth to think that periodontal disease is only caused by bacterial infection. Periodontal disease is in reality a multi-factorial disease process. Often the real cause is abnormal architecture and destructive forces that result in what Thomas Forde calls “force-induced degeneration.” In 1964 ,Thomas Forde emphatically stated in his epic book on Oral Dynamics that “Force-induced degeneration must be treated with scientific engineering principles.”
When implants arrived on the scene in the early 80s, a great deal of emphasis was placed on implant protocols that follow scientific engineering principles laid out by the inventor of the osseointegrated implant Dr. Per-Ingmar Branemark. Dr. Branemark was a true scientist who did 20 years of research before bringing implants to this country. In the beginning, practitioners followed Dr. Branemark’s recommendations carefully. In the 90s, practitioners began placing implant abutments for single teeth and small bridges as well as full arch cases. There was a veritable explosion of experimentation with various implant therapies.
Some of those therapies seem to completely disregard engineering principles—especially when implant cases are stretched beyond the limits of what they are designed for. I had the great pleasure of editing Dr. Carl Misch’s last scientific article for a dental publication. He was a scientist and expert researcher who specialized in the scientific engineering of implant fixtures and restorations. In his article “The Key to Implant Treatment Plans: Stress Treatment Theorem for Implant Dentistry” [Implant Prosthodontics Monographs; Vol 1, No. 2; June 2017], Dr. Misch emphasizes that:
“Treatment related to the science of implant dentistry should be centered around the biomechanical management of stress.”
Since implants are feats of engineering, it stands to reason that they must be handled with sound engineering principles. Dr. Misch makes it quite clear in his article that implants must be placed properly to support the restorations and the restorations must be designed so as not to overload those implants.
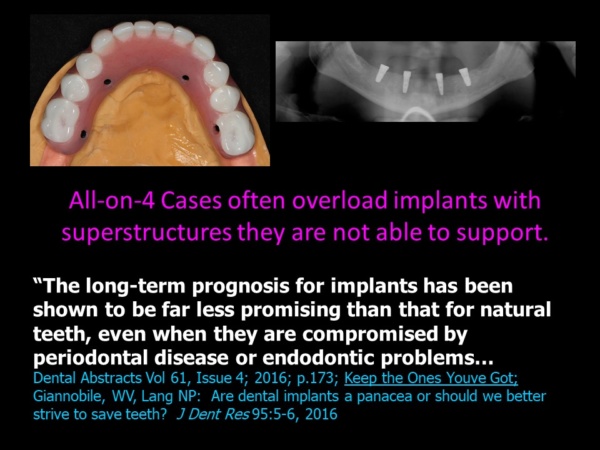 Yet the dental magazines and reconstructive seminars regularly feature oversized superstructures on implants that clearly aren’t adequate to support them. Implant patients are often missing periodontal structures (gingiva and bone) in addition to teeth and the missing anatomy is often replaced with large superstructures that overload the implants. To make matters worse, hygiene under theses superstructures is virtually impossible. It is no wonder that implant restorations are gaining a reputation for engineering failure, even though individual implants have a high degree of success initially integrating with the bone.
Yet the dental magazines and reconstructive seminars regularly feature oversized superstructures on implants that clearly aren’t adequate to support them. Implant patients are often missing periodontal structures (gingiva and bone) in addition to teeth and the missing anatomy is often replaced with large superstructures that overload the implants. To make matters worse, hygiene under theses superstructures is virtually impossible. It is no wonder that implant restorations are gaining a reputation for engineering failure, even though individual implants have a high degree of success initially integrating with the bone.
Dental cases are expensive—especially when precious metals are used, and patients are often reaching financially in order to afford that Dentistry. It is a real tragedy for them when their cases fail. Doctors are obligated to choose the type of implant restorative case that has the best chance for longevity and design that case in accordance with sound engineering principles. There can never be “one size fits all” because individuals vary widely in anatomy and physiology.
 What is clear is that dentists who incorporate sound engineering principles into their dental restorations are chasing excellence. They are meticulous in measuring their restorations and hand carving them so that they are ideal. These practitioners stand at the top end of the bell curve.
What is clear is that dentists who incorporate sound engineering principles into their dental restorations are chasing excellence. They are meticulous in measuring their restorations and hand carving them so that they are ideal. These practitioners stand at the top end of the bell curve.
Engineering principles, however, often take a back seat to productivity and profitability among average practitioners. They rarely measure or hand-carve restorations. Often the laboratory work is inserted “as is.” This protocol cannot possibly yield the same percentage of success and longevity.
“What is troubling is not just being average, but settling for it,” explains Atul Gawande, in his book Better. Details matter! But chasing excellence doesn’t mean turning into a neurotic perfectionist. True perfection is never really attainable. But, as Vince Lombardy says, “if we chase perfection, we can catch excellence.”
Chasing excellence in full coverage restorative dentistry begins with adhering to sound principles of engineering.
Become the best practitioner in full coverage restorative dentistry that you can be! Don’t settle! Join the ONWARD program and learn how to do crown and bridgework with excellence and confidence, how to save “hopeless” teeth, and how to provide new options for patient treatment that you never thought of. Visit the website and join here: https://theonwardprogram.com/membership/
Dr. Feinberg is also available to give presentations. His CV and speaker packet is posted on the website. Dr. Feinberg can be reached at info@theONWARDprogram.com
You may also like
Some Thoughts on Scientific Peer Review
February 4, 2026


A Milling Participant
December 2, 2022