Some Thoughts on the Direction of Dental Prosthetic Education
It has been my observation that the current generation of dentists is poorly prepared in full coverage restorative dentistry in dental school. It is my observation that full coverage concepts in dental institutions of higher learning have proven to be incorrect much of the time. Prosthodontic education is going in the WRONG direction. I know that my perspective is a minority opinion. However, my background hails from the roots of prosthodontics, and I have 70 years of documented evidence to back my opinion.
I believe that the profession took a wrong turn when dental educators wanted to teach students concepts and techniques that they deemed “easier.” In all fairness, dental educators have to ensure that dental students can do SOMETHING when they graduate. But they neglected to tell students the truth about the techniques they are teaching: that there are other techniques that are superior, and that their education actually begins on the day of graduation. As a result, prosthodontic education has become more of an indoctrination than an initiation in education. No one ever questions indoctrinated practices from dental school, and as a result, most dentists never develop critical thinking skills.
The professors also believe that they are adequately preparing students because they provide access to high technology right off the bat. With this approach, however, students never learn how to apply basic concepts in all dental environments. They never grasp the fact that technology is only a tool and not an end in itself. In all probability dental students will not have access to high technology in residency programs. What will they do there? They will be poorly equipped to take care of those patients.
Residents and recent graduates do not understand that some of the new technologies that they are quick to embrace actually violate basic principles of science and engineering known to contribute to successful outcomes. They have no idea that many of the problems that they experience with full coverage restorative dentistry–such as recurrent decay and loss of retention–were actually solved in the 1930s! I have noticed that—of late–there seems to be a general fear of preparing teeth for simple crowns and bridges. I have even witnessed instructors from well-known institutes recommend complicated treatments when a simple, tried-and-true six-unit anterior bridge would deliver the best esthetic result with the least amount of invasiveness!
Many dentists today have excellent implant skills, but poor crown and bridge skills, and implant therapy has proven to be quite lucrative. New graduates are under a great deal of pressure to earn money. Many graduate with debts of half a million dollars or more. At a time when they SHOULD be concentrating on building their knowledge and skills, they are forced to think about repaying loans. It’s no small wonder, therefore, that most dentists would rather place implants than save teeth. There is an absolute epidemic of tooth extraction and implant placement, and implants are being overused and used inappropriately. The sad reality is that many teeth currently being extracted can EASILY be saved.
I believe that patients want choices. They want their doctors to excel at crowns and bridgework on natural teeth as well as on implants. In actual practice patients are rarely offered choices because few practitioners can offer them. Who wouldn’t want to save their own teeth first? Implant therapy should be considered as a last resort (except in certain circumstances), not as a first resort.
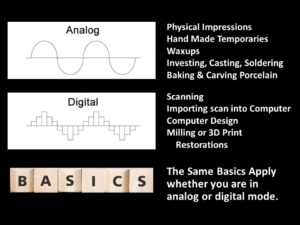 New graduates also harbor a mistaken perception that “digital” is always superior to “analog.” This might be true in the future, but it certainly is not true at the present time. In fact, the best outcomes today probably involve a blend of both analog and digital techniques. My observation is that—sadly–the current generation can actually do quite a bit less with digital than their forbears did with analog. Is this progress? I think not!
New graduates also harbor a mistaken perception that “digital” is always superior to “analog.” This might be true in the future, but it certainly is not true at the present time. In fact, the best outcomes today probably involve a blend of both analog and digital techniques. My observation is that—sadly–the current generation can actually do quite a bit less with digital than their forbears did with analog. Is this progress? I think not!
I believe that it is important to have “analog” skills first, and that these skills will transfer easily to digital concepts. However, since dental students no longer do laboratory work, they have poor “analog” skills. Without a strong understanding of analog basic principles, do dental educators really think they can develop a strong understanding of digital techniques? Not likely. The proof can be seen in the work produced by most dental laboratories. Almost all restorations they produce are oversized—and dentists overwhelmingly accept them! No one is measuring restoration thickness on vital teeth with an Iwansen gauge. No one pays attention to Carl Misch’s stress treatment theorem, which states that implant treatment must be centered around the biomechanical management of stress. Oversized restorations apply excessive stress to the periodontal foundation, and excessive stress contributes to periodontal and peri-implant bone loss.
 I believe whole-heartedly that in order to scientifically progress, anything new that comes down the pike MUST be compared to the standard of what came before. This is NOT being done. As a result, the current generation also has no idea how to evaluate digital technologies to determine whether they are good or bad. They only know how to evaluate technology from the perspective of “workflow” and “economics,” not from the perspective of longevity and health.
I believe whole-heartedly that in order to scientifically progress, anything new that comes down the pike MUST be compared to the standard of what came before. This is NOT being done. As a result, the current generation also has no idea how to evaluate digital technologies to determine whether they are good or bad. They only know how to evaluate technology from the perspective of “workflow” and “economics,” not from the perspective of longevity and health.
Young practitioners today are being conditioned to seek out the “fast” and the “easy.” They want “shortcuts” and “cookbook recipes” that do not involve critical thinking. The reality is that the ”quick-fix, quick-buck” approach to delivering dental care can never deliver a high-quality outcome. Quality demands critical thinking, attention to detail, and diligent application of step-by-step protocols that correct errors before they are compounded.
It is my observation that the current generation of dentists does not respect the clinical experience of older practitioners. Many young practitioners have the attitude that they actually know more than older practitioners who have decades of clinical experience. After all, they are adept at using computers while older practitioners use “old-fashioned” techniques. Some younger practitioners actually believe that older practitioners are not needed, since any knowledge or skills that they need can be obtained by watching YouTube videos. Nothing could be further from the truth, and they will be the ones who suffer in the end. How do you change such an ingrained and erroneous mindset? Damned if I know. Decades of evidence and merit don’t seem to matter very much these days.
 When I was a resident, my fellow residents and I were so eager to learn from experienced dentists. We knew that we knew nothing, and we would have done anything to learn from them. We were—at the drop of a hat–available evenings and weekends whenever free CE was being offered. But today’s generation values time off more than it values free CE. I once offered to give an all-day course to a residency program on a Saturday at my own expense. I was told that the residents would NEVER come on their day off. I have heard lots of complaints about the attitudes of residents from attending dentists I have met.
When I was a resident, my fellow residents and I were so eager to learn from experienced dentists. We knew that we knew nothing, and we would have done anything to learn from them. We were—at the drop of a hat–available evenings and weekends whenever free CE was being offered. But today’s generation values time off more than it values free CE. I once offered to give an all-day course to a residency program on a Saturday at my own expense. I was told that the residents would NEVER come on their day off. I have heard lots of complaints about the attitudes of residents from attending dentists I have met.
I always thought I would be a mentor to a young practitioner, since I had an amazing mentor who made me what I am. I have a lot to give. At the beginning of my career, my colleagues would have given their “eye teeth” to have someone like me in their practices willing to teach them everything. I have yet to find a single young practitioner today who would welcome my mentorship—and this is equally true for both New York and Arizona. This reality has been very tough for me to swallow! I care deeply about the future of my profession, and I am watching Dentistry’s reputation flushed down the toilet.
I am well aware that my opinion is not popular—and it is certainly not mainstream. Who would dare to say what I have just said? I’m sure some would accuse me of bias and generation-bashing, although that is not my intention. Worse yet, I am not a household name and I have no special academic titles. Why should someone like me have influence?
Because I am right. I have been blessed with the ability to accomplish miracles as a result of the knowledge that I have acquired over the course of my career. I know where full coverage dentistry came from, and I see standards re-gressing rather than pro-gressing. Full coverage restorative dentistry is on a runaway train that has seriously derailed off-track. Someone has to apply the brakes and reverse course. Given my unique background, that someone has to be me. I have unwittingly become the “gadfly” of prosthodontic education.
 Maybe it is insanity to think that one person could actually change the world. I often feel as though I am screaming into the wind and that no one is listening. (Isn’t that the very definition of insanity—screaming over and over again into the wind and expecting a different result?) But I just can’t ignore what I see and say nothing. I would be remiss if I didn’t at least try to raise the standard of care to where it should be. I care deeply about the future of my profession, so I will continue to speak out until someone does listen. I take comfort in the words of Steve Jobs: “The ones who are crazy enough to think that they can change the world are the ones who do.”
Maybe it is insanity to think that one person could actually change the world. I often feel as though I am screaming into the wind and that no one is listening. (Isn’t that the very definition of insanity—screaming over and over again into the wind and expecting a different result?) But I just can’t ignore what I see and say nothing. I would be remiss if I didn’t at least try to raise the standard of care to where it should be. I care deeply about the future of my profession, so I will continue to speak out until someone does listen. I take comfort in the words of Steve Jobs: “The ones who are crazy enough to think that they can change the world are the ones who do.”
You may also like

The Twelve Blogs of 2025

Some Thoughts on Standards