The Direction of Full Coverage Restorative Dentistry is Backward—Not Forward!
Over the course of my career, I have seen several disturbing trends in my area of dentistry—full coverage restorative dentistry (this is not true for other disciplines within dentistry like Orthodontics, Oral Surgery, and Endodontics):
-
The adoption of false beliefs based on unproven academic hypotheses.
-
The mainstream acceptance of techniques that do not compare to the standard of what came from Dentistry’s roots.
-
The deviation from a high standard of precision to a low standard of mass production and mediocrity.
-
The wholehearted embrace of technology that violates basic principles of success and longevity.
I know where Full Coverage Restorative Dentistry came from because I was raised in that discipline. Because I come from Dentistry’s “roots,” I can see clearly where it is going, and it is clearly going in the WRONG direction. I am the lone voice screaming into the wilderness.
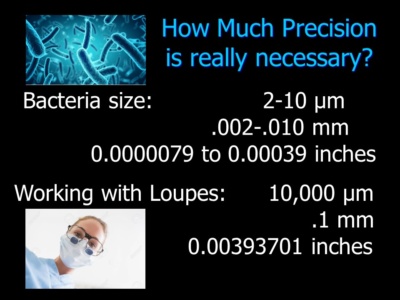
I was the protégé of a true master and pioneer—Dr. Elliot Feinberg, who was the protégé of Dr. I. Franklin Miller. It was instilled in me by my tough taskmaster to seek perfection through a precision mindset and a proven step-by-step protocol. The protocol is designed to identify and correct errors at each step to ensure a perfect, ideal result that has the best chance of lasting in health. Bacteria are microns, so errors will sabotage the final outcome.
Very few dentists are being trained to work with a precision mindset like I was trained. Instead, they are trained for speed and efficiency, to maximize production and profits. Most practitioners as a rule skip steps; and practitioners often overlook errors with false justifications of “that’s the best I can do;” or “the bonding will compensate for errors.” I have often been told, “No one can work like you do.” This is just an excuse to accept mediocrity.
My father often said that one of the hardest skills to learn was to “be your own worst critic.” I saw him redo work that 99% of Dentists would have accepted. If it is anything that I have learned it is that bacteria are microns and errors are likely to result in poor outcomes—especially in patients who are susceptible to decay or compromised with diseases like diabetes, heart disease and cancer. Only a precision approach will offer the highest percentage of case success.
What is precision? Precision is “a measure of how much detailed information is given and the degree to which exactness is applied.” [https://byjus.com/maths/precision/]. Accuracy is defined as “the measure of correctness of the value in correlation with the information.”
For example, most impression materials are quite accurate—some perhaps too accurate in the sense that they produce castings that may be too tight. However, most impressions that dentists take do not register the entire root surface. These impressions are not individual impressions of prepared teeth, they are impressions of multiple prepared teeth. This approach is not precision dentistry despite what many practitioners think.
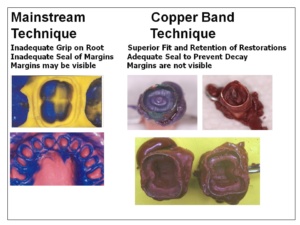 In a step-by-step precision technique, individual impressions are taken (with copper bands) that register the entire root surface. The impression must be sharp and free of tissue inclusions. With a precision approach, any impression that is not sharp or registers the entire root surface of acceptable length is never accepted. All castings are created individually and tried in to verify fit. If they are to be connected, they are connected in the mouth; and the fit of connected castings is verified in the mouth before any porcelain is baked. When no steps are skipped an ideal outcome is predictable because it is the usual result.
In a step-by-step precision technique, individual impressions are taken (with copper bands) that register the entire root surface. The impression must be sharp and free of tissue inclusions. With a precision approach, any impression that is not sharp or registers the entire root surface of acceptable length is never accepted. All castings are created individually and tried in to verify fit. If they are to be connected, they are connected in the mouth; and the fit of connected castings is verified in the mouth before any porcelain is baked. When no steps are skipped an ideal outcome is predictable because it is the usual result.
However, the overwhelming majority of dentists do not work this way. The cord impression technique does not allow for registering impressions of the entire root surfaces. The cord-impression technique usually includes multiple teeth in one impression and a one-piece casting is made from that impression. Often the casting is baked and finished at the laboratory before it is ever tried in the mouth to verify fit. This restoration may “go on” but it does not have the same accuracy of fit as the precision approach taught by ONWARD.
It is common to see roundhouses or a one-piece restoration that restores a full arch of teeth at seminars and in magazine articles. A roundhouse is NOT precision dentistry. It is impossible to prepare teeth on both sides of an arch so that they are exactly parallel. In addition, the materials are not designed for large bridges like roundhouses—they are designed for smaller bridges of 4 to 6 teeth. Distortion and errors are likely to occur with large restorations that can be clinically significant.

The new technology is certainly not designed for the level of precision taught by the ONWARD program. Scanning is confined to tooth structure above the gingiva and most of the materials like Zirconia and all-ceramic restorations are difficult to work with and confined to butt joints. A butt joint is a restoration that ends on the ledge of the prepared tooth and does not extend onto the root surface. It has been known since the 1930’s that butt joint restorations have a high incidence of recurrent decay because they can not be sealed at the micron level. Bonding is technique sensitive and it is impossible to know if the preparation is actually sealed at the micron level.
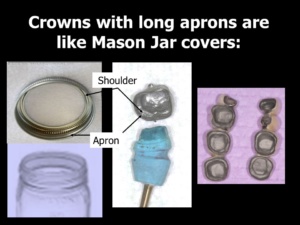 With the precision approach, crowns are designed on the model of the Mason Jar Cover, which is the best-known method of preserving food by keeping bacteria from entering the jar. Like Mason Jar Covers, restorations extend beyond the ledge onto the root surface on uncut tooth structure. This technique, which comes from the roots of Dentistry, compensates for errors that occur with laboratory techniques and actually seal the preparations. Recurrent decay under precision-designed crowns is a rarity.
With the precision approach, crowns are designed on the model of the Mason Jar Cover, which is the best-known method of preserving food by keeping bacteria from entering the jar. Like Mason Jar Covers, restorations extend beyond the ledge onto the root surface on uncut tooth structure. This technique, which comes from the roots of Dentistry, compensates for errors that occur with laboratory techniques and actually seal the preparations. Recurrent decay under precision-designed crowns is a rarity.
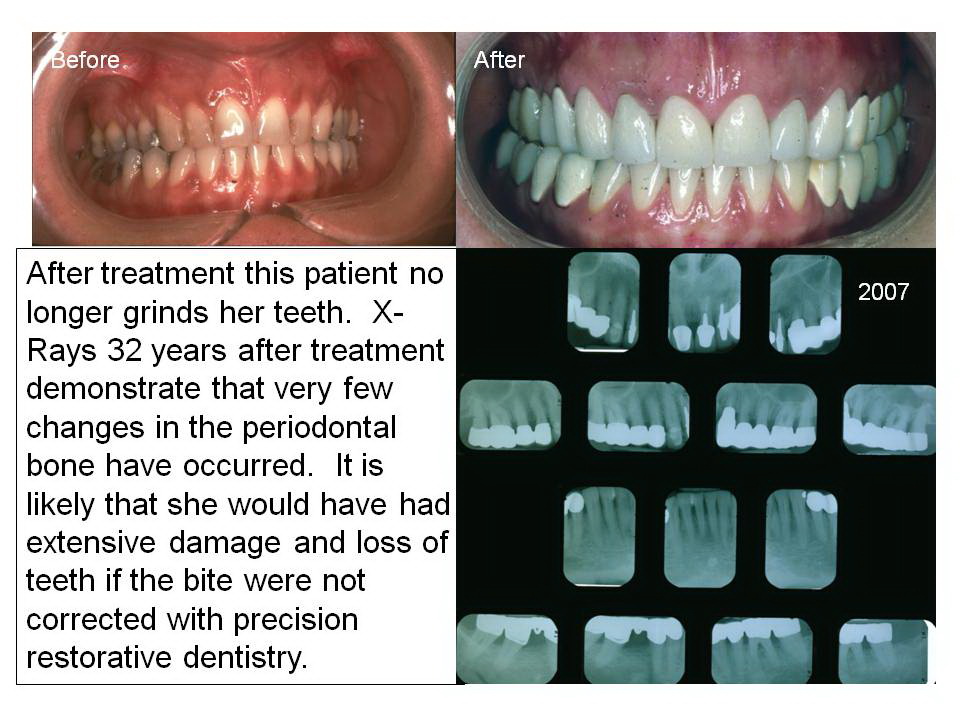 Dentists have been indoctrinated with false academic beliefs that preclude them believing that this approach is even possible! The evidence that their beliefs are incorrect is OVERWHELMING and supported by 70 years of clinical cases where all the teeth were prepared and handled in the same way. Even though these cases demonstrate close proximity to the bone in finished X-Rays, there is no violation of biologic width. If there was such a violation, healthy gingiva around these cases would not be evident and cases would not be lasting in health for decades.
Dentists have been indoctrinated with false academic beliefs that preclude them believing that this approach is even possible! The evidence that their beliefs are incorrect is OVERWHELMING and supported by 70 years of clinical cases where all the teeth were prepared and handled in the same way. Even though these cases demonstrate close proximity to the bone in finished X-Rays, there is no violation of biologic width. If there was such a violation, healthy gingiva around these cases would not be evident and cases would not be lasting in health for decades.
Somewhere in dental education, educators adopted techniques that they thought would be easier for students to accomplish. In all fairness, they have to teach students something so that they will have minimal proficiency upon graduation. But they neglected to inform them the techniques they have learned are not the only techniques and that they are not even the best techniques. They also do not instill in students the importance of precision mindset. Certain antiquated procedures like gold foil restorations had the one benefit of training students to adopt a precision mindset. They are no longer taught in the dental schools.
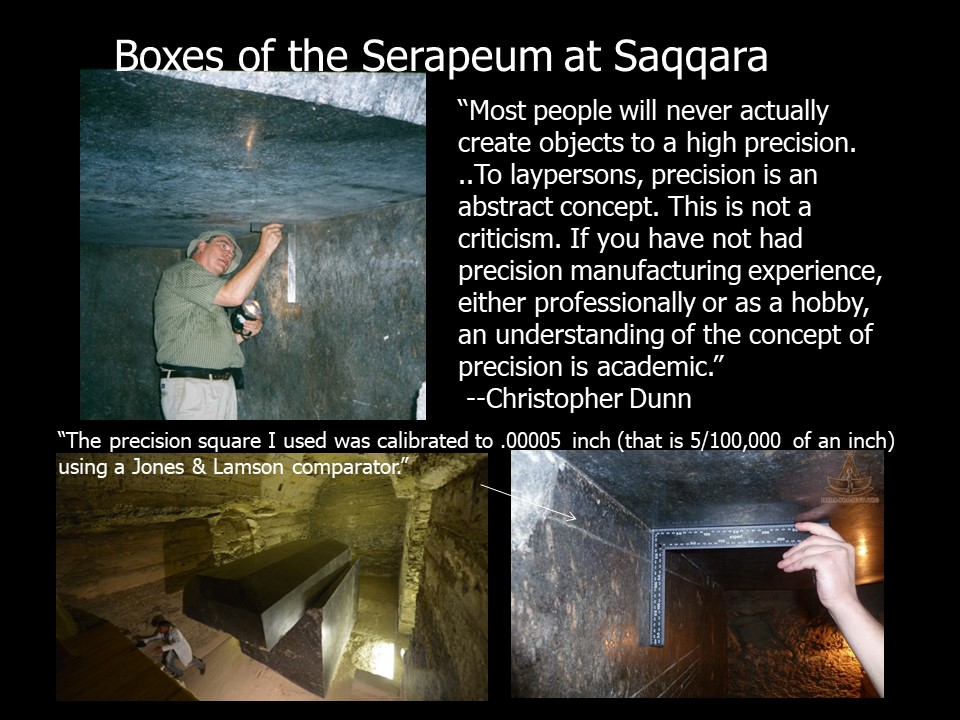
The Ancient Egyptians created objects with incredible precision. They knew that precision designs are long-lasting.
Corporations—whose only concern is bottom-line sales—has taken advantage of young practitioners who do not have an appropriate background to truly evaluate that technology. Young practitioners have a false idea that high technology is always better and more efficient than “low tech.” There also seems to be a reluctance of young practitioners to do any laboratory work and get their hands dirty. They never really learn to make their own temporaries from scratch or to use their temporaries as blueprints for the finished restorations. As a result, they are easy prey for dental companies to sell that $100,000 machine that will fabricate quick in-office butt-joint milled restorations. The patients are completely mesmerized by the technology and have no idea what they are actually getting.
What patients are, in fact, getting, is dentistry made to a much lower standard than that which was made in the past. I have the pictures that prove this premise. My father and my father’s teacher made dentistry to a much higher standard that most practitioners today could never attain—even with the fanciest cool technology. Many of these cases accomplished miracles with weak mouths and lasted in health for decades. Do you think today’s full coverage restorative techniques are an advancement? I know they are NOT.
I believe strongly that anything new that comes down the pike MUST be compared to the standard that came before. This is not being done. The question is, how can we turn this around? How can we get the profession to listen? How can we get younger dentists to adopt a precision mindset and seek excellence?
Changing attitudes is a gargantuan task that may be impossible to achieve. The academics who created easier techniques for their students actually created a monster that will not be easily tamed.
Become the best practitioner in full coverage restorative dentistry that you can be! Don’t settle! Join the ONWARD program and learn how to do crown and bridgework with excellence and confidence, how to save “hopeless” teeth, and how to provide new options for patient treatment that you never thought of. Visit the website and join here: https://theonwardprogram.com/membership/
Dr. Feinberg is also available to give presentations. His CV and speaker packet is posted on the website. (https://theonwardprogram.com/about-dr-feinberg/) Dr. Feinberg can be reached at info@theONWARDprogram.com.
You may also like

Some Thoughts on Standards
April 6, 2025

The Unspoken Conflict of Interest
March 5, 2025

Dental Social Media Groups: Bastions of “Groupthink”
January 1, 2025