
What is Fueling the Explosion of Dental Implants in the Dental Profession?
Recently I had an elderly patient who came to me in hysterics. She was told by a dentist that she had to have all of her upper teeth extracted and implants placed. She forwarded her recent X-Rays, and I examined them. Except for decay on a few teeth, she had a good mouth. It was clear to me that she certainly did not require such invasive treatment to restore her mouth. I could easily save her teeth with crown and bridgework, as she was given a great foundation for dentistry by God—good, long roots and excellent periodontal bone. What is truly upsetting is that this is not the first time I have encountered this scenario.
I cannot help but wonder what kind of doctor could propose such invasive and unnecessary treatment to a human being. It is appalling to think some doctors do not stop to consider the Hippocratic Oath: “First, do no harm.” These practitioners look at patients as if they were merely cash dispensing mannequins. They reflect negatively on all the conscientious doctors who strive to help humanity.
Dentists have differing ethical standards
 Unfortunately, dental practitioners do not seem to share the same moral compass. Ethicist Michael Josephson commented that “it’s the need to win, to be clever and to be successful in other people’s eyes that sometimes causes people to sacrifice the fundamental ideals that motivated them to the enterprise in the first place1.” It seems that very few people use ethics to weigh their actions, especially when faced with hard times. “Principles don’t do terribly well in times of fear,” notes Harry Stein, a former Ethics columnist for Esquire Magazine.
Unfortunately, dental practitioners do not seem to share the same moral compass. Ethicist Michael Josephson commented that “it’s the need to win, to be clever and to be successful in other people’s eyes that sometimes causes people to sacrifice the fundamental ideals that motivated them to the enterprise in the first place1.” It seems that very few people use ethics to weigh their actions, especially when faced with hard times. “Principles don’t do terribly well in times of fear,” notes Harry Stein, a former Ethics columnist for Esquire Magazine.
“With prices and interest and unemployment rates where they are, people aren’t feeling very secure. A lot of us are ready to do whatever we have to, to produce income, short of illegality-and some of us haven’t excluded that2.”
The fact is that most practitioners are not even aware that they are compromising ethical values. Dr. Alvin Rosenblum, an ethics professor at USC, remarked that “studies show that if an individual is asked whether he or she is ethical, that person will say yes because that is what they perceive3.” Almost no one sets out to be unethical on purpose. Unfortunately, even those who are unaware they are perpetrating questionable practices have the potential to reflect negatively on the entire profession.
Ethics is one of those subjects that is not black and white. It is often “shades of gray.” I believe strongly that dentists must always put patients first. Perhaps the best yardstick to weigh in on the ethical concerns of invasive treatment is for doctors to mentally “switch places” with the patient. Doctors should always ask themselves when treatment planning for a patient: “If you had this problem, is this what you would want for yourself? “Would you sit for the invasive procedures that you are recommending for your patient? Wouldn’t you rather save your own teeth than have implants?”
Full mouth extractions, implant placement and immediate loading with restorations is a highly invasive treatment that can be quite traumatic for patients to handle both physically and psychologically. It is much kinder to ease patients into major restorative changes, even though this approach is not financially lucrative for the dental practitioner.
Dental Continuing Education is Teeming with Implant Courses
Despite these concerns, dentists are being inundated with bold demonstrations of implant treatments in continuing education courses. Some of these treatments are quite invasive and may be considered “controversial” or “experimental,” with a long-term success rate that is unknown. I have seen instructors perform full mouth extractions of teeth that I could easily save. Most courses feature the “All-on-Four” concept that seems to be all the rage. Typically, four implant fixtures are placed in each edentulous arch. It is not uncommon for these fixtures to be immediately loaded (an experimental procedure) with large denture-like superstructures that seem impossible to clean.
Implant restorations are feats of engineering, and all engineered structures cannot be overloaded, or they will fail. There are famous accounts of bridges and buildings that collapsed when they were overloaded with forces. Don’t you think that same scenario happens in the mouth? It is not surprising that the failure rate of implant therapy is skyrocketing because implants are being over-used and used inappropriately.
 Dr. Carl Misch, a well-respected expert and researcher in implant therapy, has repeatedly warned dentists that “implant restorations must be centered around the biomechanical management of stress.” But few practitioners seem to heed his advice. Large superstructures are commonly seen restoring implant fixtures in “All-on-Four” cases at continuing education courses. Course attendees only see the esthetic result on the day of insertion. They never find out how the patients fared after they endured extractions, fixture placement and immediate loading with often arbitrarily designed restorations. Follow-up X-Rays are never shown, so attendees have no idea whether those cases were ultimately successful.
Dr. Carl Misch, a well-respected expert and researcher in implant therapy, has repeatedly warned dentists that “implant restorations must be centered around the biomechanical management of stress.” But few practitioners seem to heed his advice. Large superstructures are commonly seen restoring implant fixtures in “All-on-Four” cases at continuing education courses. Course attendees only see the esthetic result on the day of insertion. They never find out how the patients fared after they endured extractions, fixture placement and immediate loading with often arbitrarily designed restorations. Follow-up X-Rays are never shown, so attendees have no idea whether those cases were ultimately successful.
There are other methods of implant therapy that are far less invasive and ease patients into major restorative changes. These methods are rarely featured in continuing education courses, because they take longer to accomplish, are less lucrative and interfere with “workflow.”
Implants are Not a Panacea
While implants can be a godsend for many patients, they are not the answer to every restorative problem. Consider what researchers Giannobile and Lang have to say about implants:
“The long-term prognosis for implants has been shown to be far less promising than that for natural teeth, even when they are compromised by periodontal disease or endodontic problems. Often practitioners recommend implants even when teeth are only modestly compromised by caries, the need for endodontic therapy, or periodontal disease to provide the patient with a quick solution to the problem. Less trained individuals often recommend tooth extraction rather than retention. This condemns many teeth that could be treated and returned to good function. Even those teeth that are compromised have a much greater life span than the average implant4.”
Dentists are having difficulty with Crown and Bridge Procedures
One of the reasons for the immense popularity of implant therapy among dentists is that they often have great difficulty with full coverage restorations on natural teeth. The problems they are having–recurrent decay and crowns falling out–were actually solved in the 1930s! Lack of confidence with crown and bridgework is a major reason why dentists and dental educators shy away from tackling these procedures. They feel much more confident with extracting teeth and placing implants. I have seen instructors from fancy “institutes” advocate complex single tooth implants and anterior veneers when a tried and true six-unit bridge would have been the least invasive, most esthetic and quickest solution with the best prognosis for longevity!
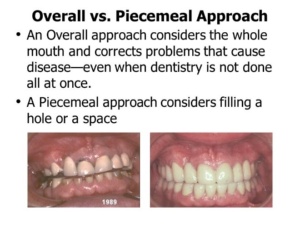 In order to achieve the best outcome, dental practitioners should be trained with an overall approach to oral health care—one that looks at the overall mouth with the idea of eradicating and preventing disease. However, most practitioners today have adopted a piecemeal approach to dental care—one that only considers filling a hole or a space. This approach does not require critical thinking and is very lucrative. The piecemeal approach is heavily supported by insurance companies, which really do not care about the patient’s overall dental health; and by implant companies who care only about selling implants.
In order to achieve the best outcome, dental practitioners should be trained with an overall approach to oral health care—one that looks at the overall mouth with the idea of eradicating and preventing disease. However, most practitioners today have adopted a piecemeal approach to dental care—one that only considers filling a hole or a space. This approach does not require critical thinking and is very lucrative. The piecemeal approach is heavily supported by insurance companies, which really do not care about the patient’s overall dental health; and by implant companies who care only about selling implants.
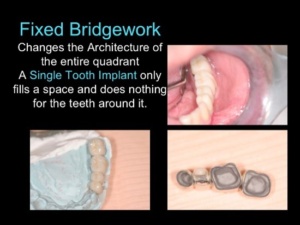
The poster child for piecemeal dentistry is the single-tooth implant, which only fills a space and does nothing for the teeth around the space. At lectures and in dental magazine articles, the teeth surrounding the implant site are rarely virginal. They have periodontal bone loss, fillings  and crowns or will likely require crowns or bridgework in the future. With the piecemeal approach, the patient’s problems are never actually solved, and the patients end up with a hodgepodge of treatments.
and crowns or will likely require crowns or bridgework in the future. With the piecemeal approach, the patient’s problems are never actually solved, and the patients end up with a hodgepodge of treatments.
Practitioners today tend to focus dental practice solely on implant therapy, so that is what every patient gets. Often the patient’s teeth are salvageable, but fewer dentists today know how to save them and fewer still have the patience for crown and bridgework procedures. These dentists are “one-trick” ponies, who often fail to provide treatment that really focusses on the best interest of their patients. Dental practitioners should remember that patients go to dentists to SAVE their teeth, not to have extractions and implants. Patients are also individuals, so there is no “one-size-fits-all.”
Patients want choices, and they want their doctors to excel at both saving teeth and providing implant therapy. The reality is that patients are rarely offered choices because few practitioners can actually offer them.
Dental School Education is Inadequate
Dentists are not educated properly from the get-go in the area of crown and bridgework. Modern techniques currently taught in the dental schools did NOT come from the roots of the profession. The original techniques had a great track record for longevity—with very little recurrent decay and loss of retention. In the 1970s, dental educators decided to teach techniques that they thought would be easier for students to accomplish. But they did not realize that the easier approach violated the basic principles that made the original techniques so successful.
Who am I to make such a statement? I have a unique background that hails from Dentistry’s roots. I was trained by a master and pioneer of full mouth reconstruction and crown and bridge dentistry—and I was trained differently than almost everyone else. I have more than 100,000 pictures of crown and bridge cases that date back to 1950—all the teeth prepared and handled the same way, and the cases followed for decades WITH X-Rays. This collection spans 70 years of documentation for these techniques. There are very definite principles that allowed my father and I (and my dad’s teacher) to have so much success, and this is what I teach on my teaching website: www.theONWARDprogram.com.
 I am able to save most teeth that dentists want to extract to place implants. I can save teeth flush with the gingiva without posts, buildups, fancy extrusion procedures or extensive crown lengthening. I am able to do so because I do not share the misconceptions and paradigms that are taught by dental educators. Dentists have been so well indoctrinated by their dental education that they believe what they were taught as gospel fact. Most are not open to learning a different paradigm.
I am able to save most teeth that dentists want to extract to place implants. I can save teeth flush with the gingiva without posts, buildups, fancy extrusion procedures or extensive crown lengthening. I am able to do so because I do not share the misconceptions and paradigms that are taught by dental educators. Dentists have been so well indoctrinated by their dental education that they believe what they were taught as gospel fact. Most are not open to learning a different paradigm.
I believe whole-heartedly that anything new that comes down the pike MUST be compared to the standard that came before. This is NOT being done in the area of prosthodontics, so it is an illusion that Dentistry is advancing in this area. There is some very cool technology recently developed for prosthodontics, but much of it violates basic principles that came from Dentistry’s roots. Technology that does not conform to basic principles of health, engineering and longevity is NOT an advancement. Dentists must recognize that technology is a tool and not an end in itself. They are responsible for the outcome of treatment, not the means by which they arrived at that outcome.
If most dentists and dental educators were properly trained, they would know that crowns and bridges are much more than “tooth coverings”! They are corrective! Only full coverage restorations have the ability to correct abnormalities; to create ideal dentitional architecture, to minimize destructive forces on the periodontal foundation (bone and roots), to prevent recurrent decay, and to minimize or eliminate periodontal bone loss. Corrective crowns and bridges compensate for periodontal bone loss to prevent future bone loss.

Corrective dentistry is possible because of Wolff’s Law, which states that bone is deposited and resorbed in accordance with the forces placed upon it. By minimizing destructive forces and compensating for periodontal bone loss, teeth solidify in their sockets and future bone loss is prevented. Periodontal disease is a multifactorial disease, and bacterial infection is only one factor. The most common factor is faulty dentitional and occlusal architecture that subjects the dentition to destructive forces. Thomas Forde, in his book The Principles and Practice of Oral  Dynamics called this destruction “force-induced degeneration” in 19645. He stated emphatically that “Forced-induced degeneration problems must be treated with scientifically proven engineering principles.”
Dynamics called this destruction “force-induced degeneration” in 19645. He stated emphatically that “Forced-induced degeneration problems must be treated with scientifically proven engineering principles.”
Corrective measures include the following:
- Correcting muscle-occlusal imbalances
- Restoring the integrity of the dental arch
- Creating an Ideal Plane of Occlusion
- Correcting faulty dentitional architecture
- Applying mechanical stress breakers such as splinting and precision attachments.
The Incursion of Corporatism into the Profession.
Corporate interests bear some of the responsibility for the absolute explosion of implant therapy in dental practice. Implant manufacturers and suppliers want to sell implants, and they are fueling the overuse and inappropriate use of implants. They are not nearly as concerned about the welfare of patients as they are about their bottom lines.
There is a disturbing increase in corporate sponsorship of implant experts at continuing education meetings. The curricula for these meetings—from major conventions to small study groups—is now overstocked with implant speakers. Crown and Bridgework experts are rarely seen on the docket of meeting programs these days. Meeting planners love to advertise that they feature speakers with no conflicts of interest, but they eagerly welcome corporate sponsorship for their events. How does this work in real life? In my opinion, it doesn’t.
Implants Definitely Have a Place in Dental Practice
Many people might think after reading this blog that I am against the use of implants, but nothing could be further from the truth. I’m against their overuse and inappropriate use. I have done many implant cases since they arrived on the scene in the early ‘80s. I recently gave a presentation and published an article (in the documents library of the website) on “Concepts for Successful Implant Therapy6.”
So, what am I for? I am for having great techniques for both implant therapy and crown and bridgework therapy for natural teeth. I am for treating patients with kindness according to the “golden rule.” I am for choosing the option that is best for each patient after considering all of the factors involved. And I am for raising the standards and level of education so that more patients can have access to the highest quality care.
©2014 Edward Feinberg DMD
1Moyers, Bill; A World of Ideas; Doubleday, 1989.
2 Stein, Harry; Ethics and Other Liabilities: Trying to Live Right in an Amoral World; St. Martin’s Press, New York; 1982.
3AGD Impact; November, 1990.
4Dental Abstracts Vol 61, Issue 4; 2016; p.173; Keep the Ones Youve Got; Giannobile, WV, Lang NP: Are dental implants a panacea or should we better strive to save teeth? J Dent Res 95:5-6, 2016.
5Forde, Thomas; The Principles and Practice of Oral Dynamics; Exposition Press, New York; 1964.
6Feinberg, Edward; “Concepts for Successful Implant Therapy;” The ONWARD program Documents Library: https://theonwardprogram.com/wp-content/uploads/2024/10/Feinberg-Concepts-for-Successful-Implant-Therapy-2024-1.pdf; 2024.
