Single Tooth Implants: The Signature of a Piecemeal Approach to Patient Care
This week’s blog is about a trend in our profession that has disturbed me for quite some time. There are less dentists today who are critical thinkers than ever before. There is a disturbing trend for dentists to adopt a piecemeal approach to dentistry rather than an overall approach to dentistry. A piecemeal approach to dentistry only looks at filling a hole or a space. Naturally the piecemeal approach is what insurance companies love to pay for. With the economic downturn, today’s dentists are looking to make a quick buck wherever they can, and they love simple, lucrative procedures that fill a hole or a space. One procedure that fulfills this desire is the single tooth implant. I think the single tooth implant is the poster child for the piecemeal approach to dentistry.
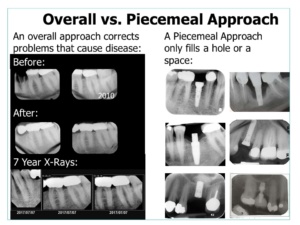
An overall approach, on the other hand, focusses on preventing disease and doing procedures that actually solve the patient’s problems, like eliminating recurrent decay and periodontal bone loss in a quadrant. I was trained to be a critical thinker, so I adopt the overall approach for everything that I do. I believe that this approach is sadly lacking in dental education. The proof is easily seen in the articles published in dental tabloids. Everyone reads the dental tabloids—and probably more dentists read these publications than scientific journals and textbooks. I admit to being guilty of this vice. In their defense, dental tabloids are extremely easy to read and have beautiful color pictures.
However, the tabloids are filled with piecemeal thinking—and how-to do quick, lucrative procedures. Dentists love these articles—and I myself enjoy seeing what is being done out there. There is no question that a tabloid article can provide dentists with some useful tips for their practices.
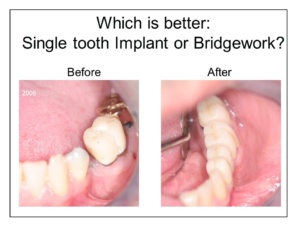
Lately, Dental Tabloids have been featuring articles on single tooth implants. The attached illustration shows examples that came from tabloid articles. A truly critical observer will notice that the teeth surrounding the implant are far from being virgin teeth. Most have big fillings, crowns or are going to need crowns. Some have obvious decay and others periodontal bone loss. The tabloids never talk about fixed bridgework as an alternative solution to the single tooth implant. While a single tooth implant is an appropriate solution if the adjacent teeth are in perfect condition, it is NOT the best solution for teeth that have already been compromised.

When making a differential diagnosis, dentists should consider these facts:
-
Ideal fixed bridgework can solve the patient’s problem for an entire quadrant, while a single tooth implant will just perpetuate the problems around the space. Fixed bridgework can prevent recurrent decay and compensate for periodontal bone loss to prevent future bone loss. A single-tooth implant cannot do this.
-
Ideal fixed bridgework has a high, predictable prognosis and is far less invasive and time consuming. Implant placement is surgical treatment.
-
Fixed bridgework immediately replaces the missing tooth when the provisional restoration is inserted. Implants usually require several months of osseointegration before a provisional restoration can be made.
-
Implants do not have a perfect track record for success and when they fail, they can leave behind huge defects in the bone that can affect the adjacent teeth.
-
Implant restorations made to fit around poor restorations and teeth with poor shape and form can lead to food impaction and periodontal problems. Fixed Bridgework prevents food impaction because the teeth are splinted.
-
Implant placement is not always ideal—even with guide stents—and poor placement can compromise the ultimate outcome.
Given these facts, does it really make any sense to thrust an implant into the bone among compromised teeth, when—for the same money—the patient will be so much better off with fixed bridgework?
I can tell you from personal experience that implants do not have the same longevity track record that bridgework has. I have had the patients where implants only lasted 20 years for reasons unknown. In a recent article in dental abstract authors Giannobile and Lang concluded that:
“The long-term prognosis for implants has been shown to be far less promising than that for natural teeth, even when they are compromised by periodontal disease or endodontic problems…Even those teeth that are compromised have a much greater life span than the average implant.” [Dental Abstracts Vol 61, Issue 4; 2016; p.173; Keep the Ones Youve Got; Giannobile, WV, Lang NP: Are dental implants a panacea or should we better strive to save teeth? J Dent Res 95:5-6, 2016]
The reason why more dentists are not doing full coverage restorations, is that they simply don’t have predictable techniques in their armentarium. “If all you have is a hammer, everything looks like a nail,” the saying goes. Few dentists know that modern techniques—including one-visit computer-generated techniques–are actually offshoots from the techniques that came from Dentistry’s roots. These techniques do not have the same track record for success because they actually violate the basic principles that gave the original techniques such a high percentage of success.
The original techniques that came from Dentistry’s roots featured gold and with acrylic veneers on the outer surfaces. Most practitioners would say today: “How unesthetic!” But before you are quick to condemn, you should realize this: Many of these restorations lasted decades, and the patients got to hold onto their teeth. Commonly, the replacement bridges for these restorations result in complications. But it is not the materials that were the responsible for the longevity of the original acrylic veneers, it was the basic principles of how they were made.
The ONWARD program teaches dentists full coverage restorative procedures that have a documented track record of great success and longevity. ONWARD’s courses are filled with cases in a library of more than 100,000 pictures of crown and bridge cases performed over a 70-year period. All of the cases were prepared according to the same basic principles, and many were followed for decades WITH X-Rays. The ONWARD program shows dentists WHY the basic principles taught eliminate recurrent decay and prevent periodontal bone loss. ONWARD techniques have a high percentage of success in patients with medical and dental compromises.
I believe strongly that if any profession is to advance, anything new that comes down the pike MUST be compared to the standard that came before. This approach to advancement should be the hallmark of every scientist. Obviously, this is NOT the case with full coverage restorative dentistry. That is why so many dentists do not have confidence in their crown and bridge techniques and why there is an absolute epidemic of tooth extraction and implant placement.
Since I’m on my soapbox, I must mention a few other pet peeves I have with dental tabloid articles. First, all of the patients featured in their publications seem to be young individuals with perfect gingiva. These patients have high tolerance and almost anything will work on them for a time. Unfortunately, most older patients cannot tolerate dental treatment shortcomings like their younger counterparts. Many have medical compromises like heart disease, diabetes and cancer that make them even less tolerant. Do the techniques promoted in the tabloids work for these patients? Few practitioners ask this question.
Readers never find out if the tabloid techniques actually worked on the young patients selected for the article. The pictures that are shown are generally taken on the day of case insertion. X-Rays are not always shown, and X-Ray/Photo follow-up is virtually non-existent. Readers never get to see if that case held up 5 or 10 years later.
I believe that five years of documentation is the minimum acceptable evidence for the efficacy of a technique. Dental Tabloid Editors should be far more demanding when they accept articles, but their objective is really to sell products and services to practicing dentists. Their current approach has been hugely successful in this endeavor; and dentists rarely raise objections in their letters to the editor.
I am hugely concerned that Dentistry will become a profession of mechanics instead of a profession of doctors. Doctors practice critical thinking according to an overall approach to patient care. They do not think in a piecemeal way because they know that piecemeal will not solve the patient’s dental problems. The objective of Doctors should not be economics and expediency first, it should be the eradication and prevention of disease. The real objective should always be to help patients save their teeth, not to replace them with implants.
You may also like

Managing Forces is the Key to Successful Implant Therapy
4 March, 2024

Which is Better: Analog or Digital?
20 December, 2023

Some Thoughts on Dentist-Laboratory Relations
3 April, 2023