Save Teeth First—Be Kind to Patients
 Last week a patient came to see me, and she was quite upset. A dentist had recommended that she have all of her lower teeth extracted and implants placed for an “All-on-Four” implant case. She has most of her lower teeth. While there was some recession, there was no mobility whatsoever and the gingiva appeared healthy. She was totally comfortable and symptom-free.
Last week a patient came to see me, and she was quite upset. A dentist had recommended that she have all of her lower teeth extracted and implants placed for an “All-on-Four” implant case. She has most of her lower teeth. While there was some recession, there was no mobility whatsoever and the gingiva appeared healthy. She was totally comfortable and symptom-free.
It is very upsetting to see dentists take advantage of patients in this manner. Such practitioners make all dentists look bad. As doctors we are supposed to help patients—and that means following the Hippocratic Oath—“First do no harm.” How would you like to be treated given the same circumstances? This question is the yardstick of how patients are to be treated.
“We’ve been wrong about what our job is in medicine [Dentistry]. We think our job is to ensure health and survival. But really it is larger than that. It is to enable well-being;” says Atul Gawande in his book Being Mortal. In order to ensure well-being, there should never be a rush to perform drastically invasive treatment. Teeth can always be extracted and there is no reason they have to be extracted immediately unless disease is present and the patient has symptoms. It is much kinder to ease patients into major restorative changes rather than plunging patients into extreme treatment. Gradual changes are much more easily accepted than drastic changes. I never saw a patient yet who was comfortable with an immediate denture (especially a lower denture, which is the worst restoration in all of Dentistry)! The immediate denture is not only physically difficult to adapt to, but psychologically difficult as well—and moreso for a young person.
If the teeth are “terminal,” it is much more prudent to fabricate a clasp partial and add teeth to it as the teeth need to be extracted. The patient will know when they are ready to have the extractions. There is no need to push them to have them sooner—no matter what X-Rays look like. Ultimately the clasp partial will be converted to a denture. At that time the patient will have choices—either a brand-new denture or implants.
Dentists must re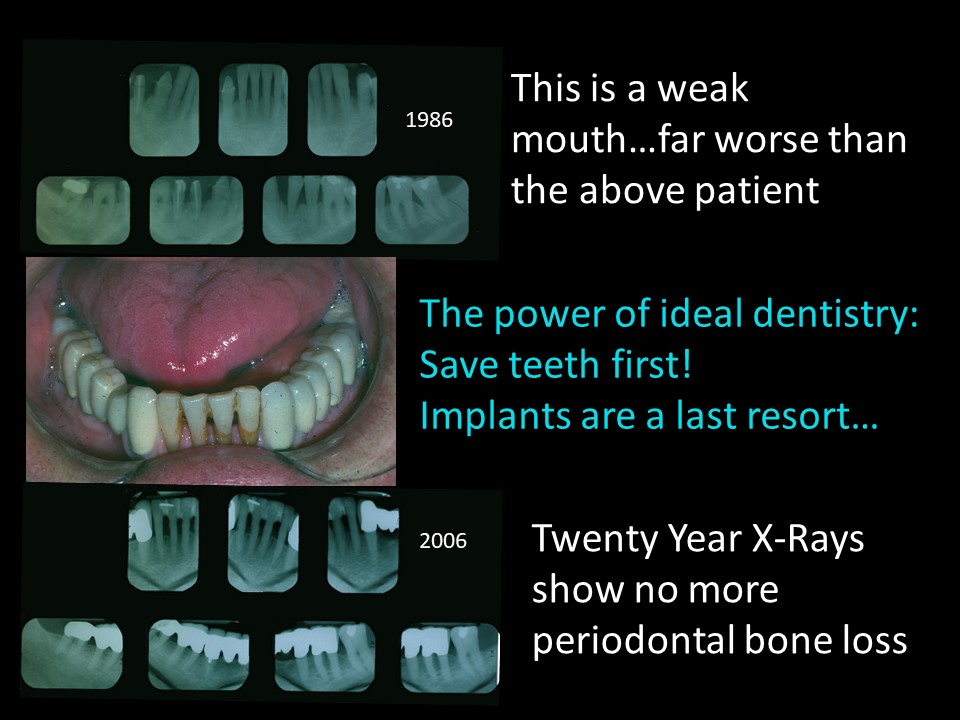 alize that “Doctor” means “Teacher.” As doctors, it is not our place to tell patients what to do or to give them only one choice. It is our duty to tell patients what is good, what is bad, what choices are available and what we recommend when they come to us for examination, diagnosis and advice. Help patients make the choices that are best for them, not the choices that will benefit us the most.
alize that “Doctor” means “Teacher.” As doctors, it is not our place to tell patients what to do or to give them only one choice. It is our duty to tell patients what is good, what is bad, what choices are available and what we recommend when they come to us for examination, diagnosis and advice. Help patients make the choices that are best for them, not the choices that will benefit us the most.
Too often Dentists do not have enough choices in their armamentarium and the patient only gets one choice—usually it is implants. Today’s dentists generally have poor crown and bridge skills, but many have excellent implant skills. For this reason, there is an absolute epidemic of tooth extraction and implant placement. I’ve been to so many lectures where the better choice for the case being shown clearly would have been crown and bridgework rather than implants. What does the patient get? You guessed it—implants.
Crown and bridgework, when done properly, offers a much more predictable result than implants. It is far less invasive and time-consuming. Full coverage restorations can solve problems, prevent recurrent decay and compensate for periodontal bone loss for an entire area, whereas implants only fill a hole or a space. The comprehensive approach is a much better strategy than a piecemeal approach. Often implants are placed with the piecemeal approach–among teeth that are falling apart, have crowns or will need crowns in the future. The patient’s problems in the area are never actually solved. Does this make sense?
My patient is comfortable and happy, even though she has some recession and bone loss. Think about how her life would change if she had all her lower teeth extracted to place an “All-on-Four” implant case. Her life would become an absolute nightmare and interfere with her self-esteem and social life. She would have difficulty accepting an immediate lower denture—the absolute worst restoration in dentistry. Almost nobody is comfortable with a permanent denture, let alone an immediate denture! The denture would most likely require a messy paste protocol to stay in place and the patient would no longer be able to chew with enough pounds of pressure to eat the foods she enjoys. The uncomfortable transition period would take several months while extraction sites heal and implants osseointegrate.
Her problems do not end there. The “All-on-Four” implant case does not have a great track record for longevity, and it is extremely expensive. When posterior implants cannot be placed deep enough in the available bone, they are often angled mesially. With this angulation implants are not only subjected to forces that do not line up with their longaxes, but they are required to support large superstructures that they are not designed to withstand.
It is important to recognize that implants are feats of engineering and as such, cannot be overloaded with forces. If one of the implants in the “All-on-Four” implant case fails, the end result is compromised, and the entire case is likely to fail. After all the discomfort, months of treatment and expense, the poor patient ends up with nothing. Carl Misch DDS MDS–one of the most famous implant researchers, states in his Stress-Treatment Theorem: “treatment related to the science of implant dentistry should be centered around the biomechanical management of stress. [Carl Misch, “The Key to Implant Treatment Plans: The Stress Treatment Theorem for Implant Dentistry;” Implant Prosthodontics Monographs; Vol. 1, No. 2; June 2017.
 There are better choices for implant therapy than the “All-on-Four” implant concept. Full-arch fixed bridgework cases should follow the Brånemark design (4-5 anterior implants with cantilevered bicuspids) or at least 7 implants (3 anteriorly and 2 posterior implants on each side) for abutment-supported anterior and posterior bridgework. These case designs have a much better track record of longevity than All-on-Four cases when implants are placed with adequate depth for support.
There are better choices for implant therapy than the “All-on-Four” implant concept. Full-arch fixed bridgework cases should follow the Brånemark design (4-5 anterior implants with cantilevered bicuspids) or at least 7 implants (3 anteriorly and 2 posterior implants on each side) for abutment-supported anterior and posterior bridgework. These case designs have a much better track record of longevity than All-on-Four cases when implants are placed with adequate depth for support.
There are many ways to manage full arch implant cases when fixed bridgework superstructures are likely to overload the implants. The Double-Tilt Precision Attachment Case can be made on three anteriorly placed implants of adequate depth: a fixed anterior bridge and posterior double-tilt precision attachment partial denture. This type of case will be covered in courses on this website in the future, but it is already covered in detail in a textbook that is available for purchase on this website.
When too much structure is missing (gingiva and bone) to support a double-tilt precision attachment case, overdenture cases are a better choice to avoid implant overload. Arian Deutsch, of Deutsch Dental Labs [https://www.deutschlab.com], fabricates the best-fitting implant overdentures that I have ever seen. He creates milled superstructures that support precisely-adapted electroformed gold copings that are embedded in the overdenture. These case designs are also likely to have a far better track record for longevity than “All-on-Four” implant cases.
In summary:
- First Do No Harm. Be Kind. Ease patients into cases that require major changes.
- Offer patients choices and help patients choose the treatments that are best for
- Design cases that minimize and balances forces on the supporting structures. Give patients cases that are most likely to succeed in longevity and health.
You may also like

Managing Forces is the Key to Successful Implant Therapy

Which is Better: Analog or Digital?
