
Full Coverage Restorative Dentistry Must Correct and Prevent Problems
It is my observation that most dentists do not appreciate the tremendous benefits of full coverage restorative dentistry can offer—both to their dental practices and to their patients. Last week’s blog pointed out how dentists commonly place single tooth implants among teeth that have or will need full coverage restorations. I believe that there is a general lack of confidence in crown and bridge skills and at the same time there is increasing confidence with implant procedures.
Unfortunately, there seems to be a lack of understanding about what full coverage restorations can do for patients. Most dentists only look at crown and bridge restorations as coverings of the teeth in the same way as a filling fills a hole or a space. However, full coverage restoration is really more like plastic surgery of the dentition.
Here’s what full coverage restorations can do for patients, aside from creating ideal esthetics:
-
Prevent Recurrent Decay
-
Compensate for Periodontal Bone Loss to prevent future bone loss
-
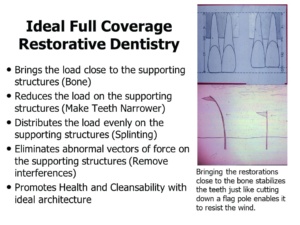
Minimize forces on the supporting structures (bone and roots)
-
Distribute forces on the supporting structures among a group of teeth through splinting
-
Eliminate Food Impaction Areas
-
Eliminate abnormal vectors of force
-
Change the alignment of the dentition in an arch
-
Create ideal architecture of individual teeth and of the dental arch
-
Promote health and cleansability of the dentition and periodontal structures
Veneers cannot do any of these; and as a result, they are fillings that cover the buccal surfaces of the teeth. Veneers and fillings can never be sealed at the micron level, where bacteria live. As a result, they are always susceptible to decay and discoloration along the margins. However, full coverage restorations done according to ONWARD techniques, seal the teeth like Mason Jar Covers and the margins are located substantially below the gingiva, so they are not visible. The Mason Jar Cover was invented in the 1830s and remains today the best-known means of food preservation against bacteria. This concept is not taught in the dental schools.
Veneers are also likely to make the teeth bigger and place more stress on periodontal structures, because veneers can only bond well to the enamel layer. It is impossible to remove enough enamel so that veneers can be fabricated to the same size as the original teeth. In older patients with periodontal bone loss, veneers are not the right treatment, because the already compromised teeth are now overloaded with forces. Full coverage restorations can be made to ideal architecture to minimize the forces and bring the forces close to the bone. Some practitioners prepare teeth for veneers like ¾ crowns, where only the lingual surfaces are unprepared. This type of preparation doesn’t make sense since the teeth are almost prepared for full crowns anyway. Wouldn’t it be better to make full crowns and have the benefits described above?
Now, it may seem like I am totally against veneers, but that is not true. I think veneers are only suitable for young people. Young individuals have teeth with very large pulp chambers, and they are more likely to require root canal therapy with standard crown and bridge preparations than older individuals, because the nerves tend to shrink during the aging process. Also, young individuals have higher tolerance than older patients and they are more likely to have less problems if the teeth are made larger with veneer restorations. There is a place for all types of restorations but is important to have a clear understanding of their limitations so they can be used appropriately.

There is one caveat, however; and that is that patients who opt for veneer preparations are committed to doing crowns one day. I doubt that many are being properly informed when they decide to have veneers. The teeth have been irreversibly cut. There will come a time when the dentistry requires replacement as dentistry is not lifetime. When that day comes, veneers will no longer be the correct treatment; the patient will require crowns.
There also seems to be a growing group of dentists who are afraid to remove tooth structure and some even specialize in minimally invasive dentistry. “Minimally invasive dentistry (MID) is an evidence-based approach that aims to arrest caries and preserve as much tooth structure as possible when managing early and moderate caries lesions.” [https://www.acffglobal.org/for-professionals/reference-materials/minimally-invasive/]. This type of dentistry is only suitable when restoring teeth with fillings. In the past, amalgam fillings required “extension for prevention” to provide adequate support for the material and remove all of the grooves and pits that could be future sites of caries. This approach is not required for bonded fillings, so extensive preparation is not required. While it is important to have respect for tooth structure and remove only what is necessary to create ideal restorations, the minimally invasive concept is not appropriate for these situations:
-
When changing the architecture of teeth is required to minimize destructive forces on the supporting structures—ie. bone and roots–and to adequately eliminate destructive food impaction areas.
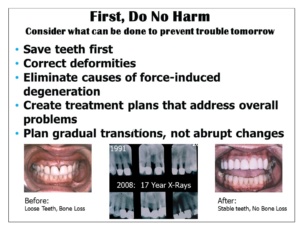
This patient was told to extract her front teeth because of the mobility and the periodontal bone loss. However, the teeth tightened up after applying basic engineering principles of design and force distribution. In 17 years there were no further changes in her X-Rays and the patient got to hold on to her teeth. -
Where adequate tooth structure must be removed in order to avoid making oversized restorations.
What good is preserving tooth structure if the teeth become in jeopardy of being lost?
Full coverage restorations, when done properly, enable patients to save their teeth first, rather than endure extractions and implant therapy. Implant therapy should always be a last resort except in certain cases. The exceptions include a virginal mouth with no decay, fillings, and periodontal bone loss; and where there are no lower teeth at all. Most people cannot tolerate the lower denture because the muscles of the tongue and cheek continually dislodge the denture. Only implant therapy can help these patients.
When practitioners have solid techniques of full coverage dentistry in their armamentariums, they can choose the best treatment plans for their patients and help them prevent future disease and tooth loss. The best feeling in the world is watching the patients come for hygiene year after year and seeing no changes in follow-up X-Rays. You did something great for those patients and they know it! They see their friends going through lots of difficulties with their teeth and they don’t have their problems! The whole point of the ONWARD program is to help dentists experience this joy—and there is no better feeling in the world than helping a patient keep their teeth for a lifetime.
All that is necessary is an open mind that is willing to learn and to set aside biases and ingrained myths and misconceptions.
You may also like

Managing Forces is the Key to Successful Implant Therapy
4 March, 2024

Which is Better: Analog or Digital?
20 December, 2023

Some Thoughts on Dentist-Laboratory Relations
3 April, 2023